SUPPLEMENTAL MATERIALS
Contents
Sample Forms and Miscellaneous
Additional Child Abuse Reading
Allegations of Sexual Abuse Amidst Divorce/Custody Disputes
Legal
2
Medical
3
Sample Forms and
Miscellaneous
4
CORNERHOUSE INTERVIEW ROOM SET-UP
SECTIONAL COUCH
Ceiling mounted camera - full picture
WALL- MOUNT- ED DRAW- ING PAD
SECTIONAL
COUCH
TRUNK WITH ANATOMICAL DOLLS
Ceiling mounted camera - picture in picture
DOOR
5
CornerHouse Intake Form (long-hand)
| Interview Date: | Medical Date: | ||
| 1st Interview Reschedule Date: |
1st Medical Reschedule Date: |
||
| 2nd Rescheduled Interview Date: |
2nd Rescheduled Medical Date: |
6
7
| ▢Physical | ▢Emotional |
| ▢Sexual | ▢Neglect |
| ▢Witness to violent crime | ▢Domestic |
8
9
10
CornerHouse
CA SCALE-CRITERIA FOR ANALYSIS*
The CA Scale combines five components to evaluate the child's statements, behaviors and emotions during a forensic interview.
Content
Consistency
Context
Ability Child's
Affect Child's
Adapted from:
Ahlquist, A. & Batko, P. (1985). Hennepin County Community Services.
11
CORNERHOUSE INTERVIEW SYNOPSIS
Name:
DOB:
Client Number:
Parent/Guardian:
Date/Time of Interview:
Videotapes:
Possession:
Interviewer:
Observers:
CC:
Date sent:
12-14
- SAMPLE -
CORNERHOUSE INTERVIEW SYNOPSIS
*All identifying information is fictional*
Name: Jenna Shane
DOB: 8/12/94
Client Number: xxxxx
Parent/Guardian: Jessie Shane
Date/Time of Interview: 6/20/01,10:30 PM
Videotapes: Yes
Possession: CornerHouse, Hennepin Co. Sheriff
Interviewer: Barb Hiltz
Observers: Det. Jim Skaja, Hennepin Co. Sheriff;
Inv. Tina Pomerleau, Osseo PD;
Becky Morrison, Hennepin Co. ACA;
Brandi Coady, CH (video technician)
REASON FOR INTERVIEW AND OTHER PERTINENT INFORMATION
Six-year, eight-month-old, Jenna Shane was referred for a CornerHouse interview by Investigator Tina Pomerleau of Osseo Police Department. According to law enforcement reports, Jenna's mother, Jessie Shane, reported that she dropped Jenna off at her parents' house (where James lives) late on 4/5/01, and picked her up late on 4/6/01. Reportedly on 4/29/01, Jenna told her mother that during that visit, James "touched her private parts" and wanted her to take off her underwear. Jenna reportedly did not do this. James then reportedly told Jenna to "rub his penis because it was hurt," which Jenna did. James also reportedly put his penis in Jenna's mouth and made her suck on it. This reportedly took place in the basement family room of James's residence. The children's grandparents reportedly found the children watching television in the middle of the night and, not realizing there was a problem, made the children go to bed.
Jenna's mother reportedly waited to report the incident because she wanted to talk to Jenna's father and because it seemed that Jenna was okay. Law enforcement recommended that Jenna have a medical examination and seek therapy (unclear if these things have been done).
James Shane was interviewed at CornerHouse as a potential victim on 5/23/01 regarding a separate allegation.
Ms. Shane brought Jenna to CornerHouse for her interview. In a brief, pre-interview meeting with Ms. Shane and Brian Mitchell (Jenna's biological father), Ms. Shane indicated that when the police came to talk to her about her allegation, Jenna would not talk to them. Ms. Shane stated that she sat on her mother's lap and would whisper the answers to the officer's questions in his ear. Ms. Shane indicated that they last talked about this alleged incident on Sunday.
INTERVIEW CONTENT
For complete information regarding this interview, please review the videotape.
Jenna presented as an extremely bright and somewhat timid six-year-old girl. Jenna wrote many of her answers to this interviewer's questions and provided the necessary verbal communication to tell of her experiences. More than once, Jenna moved to the floor and sometimes appeared to be hiding.
Jenna was interviewed using drawings, diagrams and anatomical dolls. Results of this interview appear to indicate that sexual abuse of Jenna did occur. Jenna described that James touched her private part (genitals) on her skin, and made her suck on his private (penis). Jenna provided consistent, detailed information about both events, and used the dolls to clarify the sucking of James's penis. Initially, Jenna indicated that James made her rub his penis, but provided no details of this. Jenna stated, "he's doing this to his girlfriend, too."
Jenna indicated that she was made to suck James's penis more than one time, although it was unclear if this happened on more than one occasion. Jenna described being downstairs at her grandparents' house, laying on a pillow. Jenna denied that anyone else had ever done something similar to her.
Safety messages were given.
Note: After this interview, law enforcement asked that this interviewer explain the CornerHouse medical procedure to Jenna's parents. Ms. Shane and Mr. Mitchell appeared concerned that it would be traumatic for Jenna as she had recently been seen by a general practitioner and had cried. This interviewer indicated that I would consult with Dr. Linda Thompson regarding the need for a CornerHouse exam (see CornerHouse Correspondence Form in file).
CC: Det. Jim Skaja, Hennepin Co. Sheriff's Office Inv. Tina Pomerleau, Osseo PD
Date sent:
15
INTAKE/INTERVIEWER CHECKLIST GUIDE
FOR ESSENTIAL MEDICAL EXAMINATIONS
Child's Name: __________________________________ Date: ____________
Alleged Perpetrator's Name: _____________________ Race: ____________
Adult or Juvenile: ____________________ Relationship to child: _______________
INTERVIEW RESULTS: Abuse occurred ___ Abuse Did Not Occur ___ Inconclusive ___
| YES | NO | |
| ___ | ___ | Non-acute referent request for a sexual abuse examination for purposes of providing health assessment, legal prosecution or social services intervention and investigation. |
| ___ | ___ | Skin on skin contact, or exchange of bodily fluids. |
| ___ | ___ | Report of genital trauma, discharge, bleeding, concern of STD or pregnancy. |
| ___ | ___ | CornerHouse interview conclusions are that abuse occurred and there are allegations of penetration (digital or penile, oral, vaginal, or anal). |
| ___ | ___ | CornerHouse interview conclusions are inconclusive or did not occur yet there remains concern or strong indication that the child is blocking or minimizing. |
| ___ | ___ | Child has expressed concerns about his/her body |
| ___ | ___ | Child under three years of age, or is unable to verbalize experience as a result of developmental stage. |
| ___ | ___ | CornerHouse medical examination recommended: |
| ___ | ___ | Has child reached puberty? (See below ***** footnote) Scheduled: _____________ Results: ___________________ |
| ___ | ___ | Medical examination completed elsewhere: Dr: ________________________ Results: _______________________ |
***** A separate questionnaire needs to be completed if the child has reached puberty
16
Child's Name: __________________ Date of Birth: _______________ Client Number: __________________
Child's Current Residence: _________________________________________________
Examining Physician:______________________ Exam Date/Time: ________________
Primary Physician/Address: ___________________________________________________
Law Enforcement: ___________________________ Child Protection: _____________________________
City: _______________ Phone: ________________ County: _______________ Phone: _________________
PERSONAL MEDICAL HISTORY
Informant/Source of Information: ____________________________________________________
Past Medical History:
_________________________________________
__________________________________________________________
__________________________________________________________
Immunizations Current? [ ] Yes [ ] No [ ] Unknown
Describe:
___________________________________________________________
___________________________________________________________________
Allergies: _____________________________________________________
Current Medications: _____________________________________________________
Previous Abuse? [ ] Yes [ ] No [ ] Unknown
Describe:
___________________________________________________________
___________________________________________________________________
Previous History of Anal/Genital Injuries, Surgeries,
Diagnostic Procedures,
or Medical Treatment?
[ ] Yes
[ ] No
[ ] Unknown
Describe:
___________________________________________________________
___________________________________________________________________
Has Patient Been Sexually Active? [ ] Yes [ ] No [ ] NA
Date/Time of Last Voluntary Intercourse: ______________________________
Does Patient Use Contraceptives? [ ] Yes [ ] No [ ] NA
If YES, Describe: _________________________________________
17
Previous Pregnancies? [ ] Yes [ ] No [ ] NA
Date of Last Menstrual Period: ________________ Average Length: ____________________
Menstrual Irregularities: ________________________________________________________
DESCRIPTION OF ABUSE
[ ] See Interview Report and Description
[ ] Oral Report from CornerHouse Interviewer: __________________________________
Interviewer Description:
________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
Parent Description:
________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
Child's Description:
________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
18-19
More Than 72 Hours Since Incident(s) [ ] Yes [ ] No [ ] Unknown
Parent Present During Exam? [ ] Yes [ ] No
Medical Assistant Present During Exam? [ ] Yes [ ] No If so, name: ______________
Medical Resident Present During Exam? [ ] Yes [ ] No If so, name: ______________
| Patient | Historian | ||||||||||
| Physical Symptoms | Y | N | U | NA | Y | N | U | NA | Description | ||
| Abdominal Pain | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Pelvic Pain | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Enuresis Day | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Enuresis Night | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Genital Itching | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Genital Discomfort/Pain | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Genital Discharge | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Genital Bleeding | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Rectal Pain | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Rectal Bleeding | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Rectal Discharge | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Constipation | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Incontinent of Stool | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Physical Injuries | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Other Somatic Complaints | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Behavior/Emotion Symptoms | |||||||||||
| Eating Disturbances | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| School Problems | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Sexual Acting Out | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Fear | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Anger | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Anger | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Depression | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
| Other Symptoms | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | [ ] | |||
Child Receiving Counseling: _________________________________________
Comments and Reactions of Child During Exam:
__________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
20
PHYSICAL EXAMINATION
Describe and Draw Physical Injuries in Detail (Use Drawing on Attached Page to Detail Injuries).
Weight(kg): _________________ Height(cm): __________________
| Normal | Abnormal | ||
| HEENT: | [ ] | [ ] | Description: ________________________________________ |
| Neck: | [ ] | [ ] | Description: ________________________________________ |
| Heart: | [ ] | [ ] | Description: ________________________________________ |
| Chest: | [ ] | [ ] | Description: ________________________________________ |
| Abdomen: | [ ] | [ ] | Description: ________________________________________ |
| Back: | [ ] | [ ] | Description: ________________________________________ |
| Buttocks: | [ ] | [ ] | Description: ________________________________________ |
| Extremities: | [ ] | [ ] | Description: ________________________________________ |
| Skin: | [ ] | [ ] | Description: ________________________________________ |
| Other: | Description: _______________________________________________________ | ||
GIRLS:
Exam Position: [ ] AP Supine [ ] Frog Leg [ ] Knee Chest [ ] Lithotomy
Exam Technique: [ ] Traction [ ] Separation
Tanner Stage: Breast: ________________ Genital: ________________
Clitoris: ________________________________________
Labia: ____________________________ Urethra:___________________________
Posterior Fourchette: ___________________________________________
Vestibule: ________________________________________________
Hymen: ____________________________________________________
Vagina: ________________________________________________
Perineum: ________________________________________________
Anus/Rectum: ___________________________________________
BOYS:
Tanner Stage: ____________________________________________
Penis: ________________________________________________
21
Scrotum/Testes: _____________________________________
Perineum: _________________________________________
Anus/Rectum: ______________________________________
Photocolposcope: [ ] Yes [ ] No Photos reviewed by: _______________ Date: ____________
LABORATORY SPECIMENS
For CHCM Lab (See Sexual Assault Lab Report for Results).
| 1. | GC Culture | Y N |
| A. Pharynx | Y N | |
| B. Cervix/Vagina | Y N | |
| C. Rectal | Y N | |
| D. Urethra (Male) | Y N | |
| 2. | Chlamydia Culture | Y N |
| A. Cervix/Vagina | Y N | |
| B. Urethra (Male) | Y N | |
| C. Rectal | Y N | |
| 3. | Pregnancy Test (Urine) | Y N |
| 4. | Routine Bacterial Culture | Y N |
| 5. | Wet Prep | Y N |
| 6. | UA/UC | Y N |
| 7. | Syphilis Screen | Y N |
| 8. | HIV Antibody | Y N |
| 9. | Hepatitis B Surface Antigen | Y N |
| 10. | Hepatitis B Antibody | Y N |
| 11. | Other | Y N |
Other Describe:
______________________________________________
____________________________________________________________
____________________________________________________________
Lab Report Reviewed: __________ Date ___________
DRAW SHAPE OF ANUS AND ANY LESIONS ON GENITALIA, PERINEUM AND BUTTOCKS:
Report of Child Sexual Abuse Exam Reveals:
*[ ] Normal Physical Findings
22
[ ] Exam Consistent with History
[ ] Exam Inconsistent with History
*[ ] Abnormal Physical Findings
[ ] Exam Consistent with History
[ ] Exam Inconsistent with History
ASSESSMENT:
RECOMMENDATIONS:
Examining Physician: _________________________ Date: __________
Print Name:_
CC:______________________________________ Date Sent:
_________________________________________
_________________________________________
23
STATE OF MINNESOTA
DISTRICT COURT
COUNTY OF HENNEPIN
FOURTH JUDICIAL DISTRICT
|
State of Minnesota, Plaintiff, vs. < > Defendant. |
STIPULATION AND OTHER SIP No. < > CA. No. < > |
* * * * * * * * * * * * * * * * * * * * *
The parties to the above-reference action stipulate to the following:
1. That a copy of a videotaped interview of a child witness shall be made available to the defense;
2. That no additional copy of the tape nor any portion of the tape shall be made by the defendant, the defendant's attorney, investigator, expert, or any other representative or agent of the defendant;
3. That said copy shall not be used for any purpose other than to prepare for the defense in the above-referenced action;
4. That said copy shall not be publicly exhibited, shown, displayed, used for educational, research or demonstrative purposes, or used in any other fashion, except in judicial proceedings in the above-referenced action;
5. That said copy may be viewed only by parties, their counsel and their counsel's employees, investigators, and experts;
6. That no transcript of said copy, nor the substance of any portion thereof, shall be divulged to any person not authorized to view the tape;
7. That no person shall be granted access to said copy, any transcription thereof, or the
24
substance of any portion thereof unless that person has first signed an agreement in writing that he or she has received a copy of this stipulation, that he or she submits to the Court's Jurisdiction with respect to it and that he or she will be subject to the Court's contempt powers for any violation of it;
8. That upon final disposition of this case, any and all copies of these tapes and any transcripts thereof shall be returned to the Hennepin County District Court.
_____________________________
Attorney for Plaintiff
Dated: _______________________
_____________________________
Attorney for Defendant
Dated: _______________________
ORDER
IT IS SO ORDERED.
Dated: _______________________
_______________________________
Judge of District Court Fourth Judicial District
25
Additional Child Abuse Reading
26
Reprinted with permission from:
Summit, R. C. (1992). Abuse of the child sexual abuse accommodation syndrome. Journal of Child Sexual Abuse. 1(4153-163
Abuse of the Child Sexual Abuse Accommodation Syndrome
Roland C. Summit, M.D.
Harbor/UCLA Medical Center,
1000 W. Carson St, D-6, Torrance, CA 90509
(310) 533-3129
Introduction
The Child Sexual Abuse Accommodation Syndrome (CSAAS) (Summit, 1983b) is a clinical observation that has become both elevated as gospel and denounced as dangerous pseudoscience. The polarization which inflames every issue of sexual abuse has been kindled further here by the exploitation of a clinical concept as ammunition for battles in court. The excess heat has been generated by false claims advanced by prosecutors as well as by a primary effort by defense interests to strip the paper of any worth or relevance. The following commentary will address the origins of the child sexual abuse accommodation concept and the subsequent distortions that court misuse has imposed. I hope that such a contextual review can serve as a guide toward a more accurate understanding among clinicians, judges, and advocate attorneys.
Background
Appeals decisions have groped for a definition of the intent and purpose of the CSAAS, assuming sometimes that it is intended for diagnosis or for substantiation of complaints. It has been presumed at times to be both an instrument and an opinion. I would propose that the answers to such questions can be found not in adversarial debate but in an examination of the origins of the CSAAS itself.
It was only when I began reviewing courtroom opinions during the late 1970's that it became apparent that prevailing clinical experience was at odds with forensic demands. From the viewpoint of a community psychiatrist specializing in sexual abuse consultation, it had become axiomatic that children were reluctant to disclose sexual victimization and that potentially protective adults were often incredulous and threatened by the implications of a child's complaint. I was surprised to discover that lawyers tended to discredit delayed and inconsistent reports, insisting that any legitimate victim would have made an immediate and convincing complaint. I began to understand that legal assumptions equating reliability of a testimony with a fresh and consistent complaint merely formalized the standoff that has always existed between victimized children and the adults in authority they must face to gain sympathy and protection. The small victim of a private crime must search against fear of rejection for the adult who will listen to an unwelcome, offensive account and take protective action against a trusted peer.
27
In the summer of 1979,1 put together a list of those factors which were both most characteristic of child sexual abuse and most provocative of rejection in the prevailing adult mythology about legitimate victims. The basis for those typical characteristics was my own broad consulting experience throughout Los Angeles County as well as personal discussion with such national visionaries as Ann Burgess, Sue Sgroi, Nicholas Groth, Lloyd Martin, Louise Armstrong, Lucy Berliner, Hank Giarretto, Kee MacFarlane, Karin Meiselman, Judith Herman, Diana Russell and, especially, David Finkelhor.
The first five of the seven factors on the original list formed a logical pattern and sequence of interaction among the victim, the intruder, and the potential caretakers. Together, these five points described both the luxury of the adult world not to listen and the accommodating efforts of the child not to complain. The factors as listed were: (1) secrecy, (2) helplessness, (3) entrapment and accommodation, (4) delayed, conflicted and unconvincing disclosure, and (5) retraction.
I began to use that pattern as an outline for lectures explaining the dynamics of sexual victimization, calling it the Child Sexual Abuse Accommodation Syndrome. The lectures had the compelling effect of helping professional and public audiences to understand, as if for the first time, how sexual abuse can occur. It became commonplace for adult survivors to seek me out after such a lecture to express gratitude that someone could understand. They typically felt relieved and forgiven, having condemned themselves as uniquely weak or bad for their uncomplaining compliance as a child.
The published record of the CSAAS begins with the transcription of an invited lecture in Victoria, British Columbia on September 29,1980 (Summit). That publication served as the basis for the text of the CSAAS which was incorporated in each of two book chapters written during the spring of 1981 (Summit, 1982,1983a). An expanded version was written during the ensuing summer and submitted to a psychiatric journal. The CSAAS was rejected, not because it was radical or unsubstantiated, but because the reviewers felt it was so basic that it contributed nothing new to the literature!
The unexpected rejection after two years of frustrating delays discouraged any further attempt at publication. Copies of the typescript continued to circulate, however, and the CSAAS took on a life of its own in progressively faded facsimile. Kee MacFarlane recommended the paper for inclusion the sexual abuse special issue of the International Journal of Child Abuse and Neglect. The typescript was reviewed, unchanged, in the spring of 1983, and finally published (Summit, 1983b).
The significance of the preceding chronology is that the CSAAS, like the labors of disclosure it seeks to describe, was not relevant to established wisdom. Even as it made sense to those with personal and immediate experience, it was unacceptable to those with gatekeeping authority. Sharing the CSAAS became centrally important to me as I tried to find the way to say it right, but on being rejected I was willing to retract it and give up. In further analogy to the plight of the child, the CSAAS depended on intervention by a sensitive, experienced professional to invite eventual disclosure.
The publication history is important also for the fact that the text of the CSAAS represents the author's experience up to the fall of 1981, more than two years before its eventual publication, with clinical anecdotes derived from consulting experience preceding 1980. The large majority of those first consultations involved incestuous abuse, which then became a convenient model for lecture presentation. Despite intervening contacts with every known
28
form of child sexual victimization, all of which reinforced the accommodation concept, the written persistence of the original anecdotes allows for the misleading impression that the accommodation phenomenon is specific to father-daughter incest. The CSAAS originated, then, not as a laboratory hypothesis or as a designated study of a defined population. It emerged as a summary of diverse clinical consulting experience, defined at the interface with paradoxical forensic reaction. It should be understood without apology that the CSAAS is a clinical opinion, not a scientific instrument.
Abuses
Contrary to its resoundingly constructive clinical reception, lawyers and a few clinical expert witnesses have tended to seize on the CSAAS as a major weapon. Adversarial rivals seem determined either to enhance it or to destroy it according to their designated role. The CSAAS posed a threat to the traditional defense arguments that legitimate victims would fight back and complain, that any good mother would know if her child were a victim, and that retractions confirm the common sense assurance that children typically lie about sexual victimization. Prosecutors saw the CSAAS as a potential offer of proof that an inconsistent victim is truthful.
Some of the adversarial alarm and distortion stems from misunderstanding of the word syndrome. In medical tradition it means a list, or pattern of otherwise unrelated factors which can alert the physician to the possibility of disorder. Such a pattern is not diagnostic, and the cause-and-effect relationship among the factors themselves and with the possible problem is generally obscure. In court circles, syndrome seems to mean a diagnosis which an expert witness contrives to prove an injury. Syndrome evidence has become a generic term for diagnostic medical or psychological testimony which must be closely scrutinized for scientific reliability, lest the intrinsic authority of the expert witness improperly prejudice a jury through contrived or eccentric opinion. Any assertion that a victim-witness or a plaintiff suffers from a disorder that was caused by the claimed injury must be tested for scientific reliability in a so-called Kelly-Frye hearing. Had I known the legal consequences of the word at the time, I might better have chosen a name like the Child Sexual Abuse Accommodation Pattern to avoid any pathological or diagnostic implications.
Despite the potential for semantic misunderstanding, it should have been obvious to a careful reader that the CSAAS was not addressing an illness or disorder. The abstract of the monograph, which was written in the summer of 1983, expresses my last and most careful epitome of what I was trying to describe:
Child victims of sexual abuse face secondary trauma in the crisis of discovery. Their attempts to reconcile their private experiences with the realities of the outer world are assaulted by the disbelief, blame and rejection they experience from adults. The normal coping behavior of the child contradicts the entrenched beliefs and expectations typically held by adults, stigmatizing the child with charges of lying, manipulating or imagining from parents, courts and clinicians...
Evaluation of the responses of normal children to sexual assault provides clear evidence that societal definitions of "normal" victim
29
behavior are inappropriate and procrustean, serving adults as mythic insulators against the child's pain. Within this climate of prejudice, the sequential survival options available to the victim further alienate the child from any hope of outside credibility or acceptance. Ironically, the child's inevitable choice of the "wrong" options reinforces and perpetuates the prejudicial myths. (1983b, p. 177, emphasis added).
These are normal children making normal adjustments to an abnormal environment. The focus is not on the effects of sexual abuse itself but on the conflict between the child's experience and the perverse indifference of the outer, adult world. If there is pathology, it is in the denial and paradoxical demands of adults, not in the survival options found by the child. The words identification, detection, diagnosis, symptom, disorder, illness and pathology, which might infer a diagnostic focus, do not appear in the paper, nor is there a promise of verifying the alleged abuse with such words as test, validate, evaluate, confirm, or prove. The accommodation mechanisms listed in the third category are obviously not specific to sexual assault. Rather, they were selected to illustrate the misleading, self-camouflaging behaviors that inhibit recognition. The CSAAS is meaningless in court discussion unless there has been a disputed disclosure, and in that instance the ultimate issue of truth is the sole responsibility of the trier of fact. The CSAAS acknowledges that there is no clinical method available to distinguish "valid" claims from "those that should be treated as fantasy or deception" (p. 189), and it gives no guidelines for discrimination.
The capacity to listen and the willingness to believe, which the paper invites, is not an
admonition to interrogate or to assume that every disclosure is real:
The purpose of this paper then, is to provide a vehicle for a more sensitive, more therapeutic response to legitimate victims of child sexual abuse and to invite more active, more effective clinical advocacy for the child within the family and within the systems of child protection and criminal justice, (p. 179-180, emphasis added).
Even the word advocacy has a loaded meaning in forensic circles. An advocate is seen as a hireling paid to advance an adversarial view, or someone with a zealous mission who cannot be objective. So the CSAAS can be read by lawyers as a rallying cry for clinicians to go forth and diagnose more children as victims, toward the goal of making more money and putting more people in jail. Whether or not attorneys saw it that way at first, that is certainly the attack directed now against the CSAAS and its alleged minions, the child advocates, or more derisively, child abuse finders or validators, who are said to be conducting a witch hunt and creating an epidemic of false allegations, launched and fueled by the SCAAS. This kill the messenger rhetoric has given the CSAAS a taint of controversy which inhibits expert witnesses from drawing on the paper as supplementary authority. Clinicians may be warned specifically by attorneys to make no reference to the CSAAS, and even to deny being influenced in their training by the views of early theorists.
When CSAAS is not stigmatized outright, it may be attacked as being irrelevant in any disclosures other than those naming the father in an intact family system. This is a frank distortion both of the scope of the CSAAS and of clinical reality. Silence is intrinsic to the
30
victimization process, not to family systems dynamics. A skillful neighborhood offender may be more immune from parental suspicion and victim disclosure than a relative. Experts who swear that a child would have no reason to conceal abuse by a teacher must be unimpressed by a case in Great Neck, NY, where a computer tutor enslaved some 400 boys and girls in pornographic exploitation and sadistic abuse over a span of 7 years with no disclosures, ever. Or the school bus driver in the same county who molested children going back and forth to school. Some 250 young children entered a bus twice a day to be molested, yet no teacher or parent heard a word of that ordeal.
While much of the destructive criticism was contrived to prevent any use of the CSAAS in court, some criticism has been a legitimate defense against improper use by prosecutors and expert witnesses called by prosecution. There has been some tendency to use the CSAAS as an offer of proof that a child has been abused. A child may be said to be suffering from or displaying the CSAAS, as if it is a malady that proves the alleged abuse. Or a child's conspicuous helplessness or silence might be said to be consistent with the CSAAS, as if not complaining proves the complaint. Some have contended that a child who retracts is a more believable victim than one who has maintained a consistent complaint. Such absurd distortions fuel the fire against the CSAAS:
Daffynition: Child Sexual Abuse Accommodation Syndrome: a brief synopsis. 1. When a child denies abuse, they have been abused. 2. When a child says they have been abused, they have been abused. 3. When a child recants an abuse, they have been abused. 4. Therefore, it is logical to conclude that all children have been abused and therefore all who have children have either abused their child or have allowed their child to have been abused. (VOCAL, 1988, p. 6).
The CSAAS is used appropriately in court testimony not to prove a child was molested but to rebut the myths which prejudice endorsement of delayed or inconsistent disclosure. Proper testimony is defined in California's People v. Gray (187 Cal. App. 3d 213: Cal. Rptr. - [Nov. 1986]). Gray translates a state Supreme Court decision into analogous guidelines for CSAAS testimony regarding child witnesses:
...Expert testimony may play a particularly useful role by disabusing the jury of some widely held misconceptions about (child sexual abuse and its) victims, so it may evaluate the evidence free of the constraints of popular myths. {People v. Gray, p. 218).
...It was not error to admit expert testimony to the effect that it was common for child victims to delay reporting of incidents of abuse and to given inconsistent accounts of such incidents to different people, where such evidence was not offered to prove that a molestation in fact occurred, but rather was offered to rebut the inference proffered by the defendant that the alleged victim was being untruthful as shown by her delay and inconsistencies in reporting, by showing that such behavior is not necessarily indicative of deceit in children. Such expert testimony was proper
31
so long as it was limited to discussion of victims as a class (e.g., children), and did not extend to discussion and diagnosis of the witness in the case at hand. (pp. 213-214, emphasis added).
Gray also defines CSAAS testimony as opinion, not scientific evidence, and therefore not subject to Kelly-Frye exclusion. "Thus, expert testimony, even where highly esoteric and controversial, is generally admissible, so long as not derived from a specific experimental or forensic procedure." (p. 214).
Reductio ad Absurdum
The ultimate barrier to CSAAS testimony is to define it as something it is not, then to bar it for its failure to meet irrelevant conditions. If the CSAAS is labeled as a diagnostic instrument, then it must undergo a Kelly-Frye hearing to demonstrate it infallibility and its general acceptance in the scientific community in which it was developed. Since the author is a psychiatrist, it is tested against the psychiatric literature and the official diagnostic and statistical manual, in which, since it is not a diagnosis, it will never appear. Working in the community gave me the privilege of learning about sexual abuse from those who knew: social workers, nurses, police, sociologists, psychologists, journalists and adult survivors. The greatest contribution from psychiatrists was an appreciation of the elitist avoidance that continues to isolate my profession from the interdisciplinary advances of child abuse awareness. The clinical expert best qualified to testify about sexual victimization is likely to be a social worker, not a physician. Yet judges persist in empowering psychiatrists with sole dominion over human behavior.
The Supreme Court of Kentucky has reversed five consecutive sexual abuse convictions involving expert witness testimony, ruling each time that the CSAAS is not a generally accepted medical concept.
However, the issue "has never been properly presented to us" said Kentucky Supreme Court Chief Justice Robert Stephens. The witnesses who testified about the syndrome were social workers and other non-medical personnel rather than traditional experts like doctors and psychiatrists, Stephens said (Nance, 1991, p. A-9).
In January the court reviewed the ultimate test case. The defendant had been condemned to 50 years in prison for molesting and sodomizing his stepdaughter over a period of six years. Expert testimony was offered by Lane Veltkamp, a full professor of psychiatry and Director of the University of Kentucky Child Abuse Center. In his 23 years of experience he had evaluated and treated over 1,000 children. His testimony avoided any reference to the CSAAS, but he was asked to comment on the child's six years of silence. He said in his experience "delayed disclosure was common among sexually abused children." The Supreme Court interpreted that statement as a reference to the CSAAS! The entire testimony was nullified and the CSAAS was scapegoated in absentia because the expert's credentials were judged inadequate to address what the court insists is medical evidence. Professor Veltkamp, medical educator and sexual abuse expert par excellence, was not to be allowed to educate a jury. The Supreme Court reversed the conviction because he is only a Master of Social Work, not a Doctor of Medicine (Nance, 1992).
32
Conclusion
It has been 13 years since I observed that victims of sexual abuse are the object of prejudice because they do not meet our artificial standards of disclosure. I thought that better education would correct this secondary abuse. The CSAAS, written to address that prejudice, was drawn from community resources and published in the interdisciplinary, international journal for child abuse awareness. Nothing in that history implies that the CSAAS is a medical issue. There are infinite behavioral variations which can be subsumed under the five categories of the CSAAS, any of which may be vital to understanding a victim's dilemma. To take all such information away from those who can best express it, to consign it to a category of medical evidence because a psychiatrist once tried to summarize it, and then to rule any and every part of such information forbidden to a trier of fact unless a physician can prove it qualified as medical evidence is the ultimate expression of the very prejudice which the courts seem so reluctant to acknowledge.
Knowledge is not enough. Education is not enough. A good clinical framework like the
CSAAS is not only not enough, it becomes worse than nothing if it offends those who are
determined not to learn. It can be used as a lock on the secret instead of the key.
The problem is not with improper use of expert testimony. The problem is not with skeptical
attorneys or recalcitrant judges; they all merely represent our continuing reluctance as an adult
society to allow an honest view of our children's continuing silence.
The answer lies not in better research or better publications. Scientific progress is no match
for prejudicial ignorance. The answer rests with broader acknowledgment that we all need to
discard familiar reassurances and struggle together for better answers. We aren't yet willing as
a society to prohibit the sexual abuse of children. Why not?
33
References
Nance, K. Supreme Court Bars Testimony on Why Children Stay Silent. Lexington Herald-Leader, December 6, 1991, p. A-9.
Nance, K. Supreme Court Overturns Sex Abuse Conviction. Lexington Herald-Leader, January 17, 1992, p. A-8.
Summit, R.C. Keynote Address. In: P.D. Ross (Ed.), Sexual Abuse of Children within the Family: Conference Proceedings (pp. Ill-1 -111-56). Vancouver, BC: Justice Institute of B.C., 1980.
Summit, R.C. Beyond Belief: The Reluctant Discovery of Incest. In: M. Kirkpatrick (Ed.), Women's Sexual Experience (pp. 127-150). New York: Plenum Press.
Summit, R.C. Recognition and Treatment of Child Sexual Abuse. In: C.
Hollingsworth (Ed.), Coping with Pediatric Illness (pp. 115-172). New York: Spectrum Publications, 1983(a).
Summit, R.C. The Child Sexual Abuse Accommodation Syndrome. Child Abuse and Neglect, 1983(b), 7:177-193.
VOCAL. Great quotes (no author cited). VOCAL's California state Newsletter. P.O. Box 1314, Orangevale, CA 95662. Sept/Oct 1988, 4(5):6.
34
Reprinted with permission from:
Vieth, V. (1994). A strategy for confronting child abuse in rural communities. The Prosecutor. Sept/Oct. 6.
A Strategy for Confronting Child Abuse in Rural Communities
Victor I. Vieth
INTRODUCTION
Recent studies conclude that children in rural communities are as likely and possibly more likely to be abused or neglected than children in metropolitan areas.1 Although rural families face the same drug, alcohol, poverty and stress problems as do families who live in cities and suburbs, rural communities typically have fewer resources.
Recognizing this crisis, the prosecutors in the Cottonwood County, Minnesota attorney's office began a vigorous attack on child abuse and neglect in 1991. This attack has proven effective for the county which has an approximate population on 13,000.
We believe it would be effective for use in other rural and small communities. Our fight against child abuse and neglect consists of six endeavors.
WRITTEN PROTOCOL
First we developed a written child abuse investigation and prosecution protocol for the county attorney's office, local welfare agency and the four law enforcement agencies serving the county.
One issue addressed in the protocol is the vacuum in child abuse expertise existing in rural communities. For instance, small police forces such as ours usually cannot afford to hire a full-time officer to handle child abuse investigations exclusively. Accordingly, the first interview of a child may be done by an on-call officer with limited training in the art of interviewing a child. To correct this problem, we decided that only one named officer or one of two named social workers would conduct interviews of young children. These three investigators would receive the bulk of child abuse framing dollars and would develop expertise in interviewing children in part by doing it more often than other investigators. A child-friendly interview room was established where interviews of young children may be videotaped for possible use in court. The protocol also seeks to involve the prosecutor early in the case. It provides that whenever the investigators believe a child abuse investigation will
1 Hopfensperger, "Rural Counties Score Lower Marks For Child Safety and Welfare." Minneapolis Star Tribune, May 9, 1994, at 1A.
35
result in criminal charges or the filing of a child protection petition, the prosecutor would "be notified regarding the basic facts of the case."2 It also provides that investigators are to "contact the county attorney's office whenever a legal or procedural question arises in an investigation and assessment."3 By involving the prosecutor early in the case, potential legal problems with a case may be avoided. For example, prosecutors can ensure that all elements of a particular charge of child abuse are investigated. In Minnesota, there may be an enhanced penalty if the perpetrator "jointly resides intermittently or regularly" in the household of the victim.4 If the perpetrator is the mother's boyfriend, it is important to determine whether the boyfriend periodically stays over or otherwise resides in the same dwelling as the victim. A prosecutor can remind an investigator of these easily forgotten elements.
If the prosecutor declines to prosecute a case of child abuse, the prosecutor must inform the investigators in writing of the reasons for the decision. In this way, investigations not resulting in charges are, nonetheless, instructive to the investigators because of the degree of evidence needed to bring a case to court.
In drafting the protocol, the prosecutors sent the message to the investigators that their efforts at combating child abuse are appreciated and will be responded to promptly. The protocol also implicitly instructs the community at large that child abuse is a top priority for police and prosecutors.
MANDATED REPORTER TRAINING
Second, we conducted mandated reporter training for public and private school teachers, day care providers, foster parents, nurses and other professionals required by law to report possible abuse or neglect.
The training of the potential reporters was conducted by the assistant county attorney and the social workers who investigate reports of abuse or neglect. The participants were given copies of Minnesota's Mandated reporting law5 and the relevant provisions were explained. In particular, focus was put on the definitions of physical abuse, sexual abuse and neglect. Also discussed were the circumstances under which a report must be made, with particular emphasis on the fact that reporting was their responsibility, and they could not comply with the law by simply informing a superior in their school or agency. The participants were informed of the need to report as soon as possible, because, if the report is received 30 minutes before the close of the school day, it is extremely difficult, if not impossible, to make a well-informed decision whether to allow a child to board the school bus or to be placed in
2 Cottonwood County Attorney's Office, Cottonwood County Protocol for the Investigation and Assessment of Child Abuse Cases. Windom, Minnesota (1993).
3 Id.
4 MINN.STAT. 609.342. 1(g) (1985): 609.343,1(g) (1985);609.341.15(3) (1985).
5 MINN.STAT. 626.556 (1975).
36
protective custody. The social workers discussed the mechanics of making a report and the process they and the police officers use in responding to a report.
One of the difficulties in protecting children in rural and small communities is that everyone knows everyone else; hence, even a mandated reporter can be reluctant to report suspicions for fear the reporter will feel uncomfortable sitting beside the alleged perpetrator at next week's ice cream social. This reluctance can be overcome by yearly training emphasizing the mandate of the law and by giving concrete examples of how the mandated reporting law has spared the lives of countless children.
SEPARATE TRAINING FOR CLERGY
Third, we conducted a separate, mandated reporter training for members of the clergy. A separate training is warranted only because most mandated reporting laws for clergy differ from mandated reporting laws for other professionals. In Minnesota, a member of the clergy is not required to report the possibility of abuse or neglect if the information is obtained while receiving a confession or from a person seeking "religious or spiritual advice."6
This law is discussed in detail with the clergy and numerous examples are given them. For example, if a pastor is visiting a parishioner in the hospital and the parishioner laments about the abuse of a given child, the pastor has received information not obtained during a confession or from someone seeking religious or spiritual advice. In their training of the clergy, the social workers gave the pastors information on behavior and other characteristics of abused children so they can better protect children in their congregations. The members of the clergy were also given information on counseling and other services in our area to which they may direct parishioners facing a particular crisis.
A separate training for pastors is a necessary reflection of the vital role they play in rural communities. Often times, the most respected leaders in these communities do not occupy a position on the school or township board; instead, they preach from a pulpit. Moreover, rural families in crisis typically do not call social services; these families may call their pastor or priest.
When local ministers are enlisted in the fight against child abuse, victory becomes foreseeable. Often times, these ministers see social workers, police officers and prosecutors as part of a government which breaks up families. By helping them understand that families involved in child abuse are already broken, and that investigators are dedicated, caring professionals, we build a bridge over which hurting children may cross and find comfort.
INVOLVING DOCTORS
Fourth, we hired a pediatrician dealing exclusively with cases of child abuse to conduct an advanced training for local doctors in the art of detecting abuse. Because small town doctors
6 MN STAT. 626.556.3(a)(@)(1984); 595.02 1© (1984).
37
are, by necessity, general practitioners, it is vital to give these professionals specialized training on detecting child abuse. Our physicians were trained in the use of a colposcope in the examination of a child victim of sexual abuse. Long-bone fractures and other tell-tale signs of abuse were also discussed. To accommodate their schedules, we conducted our training as an early morning breakfast for our doctors. This accommodation, and the training itself, were well received.
CULTURAL DIVERSITY TRAINING
Fifth, we conducted, in conjunction with other groups, a cultural diversity training program for all interested social workers, police officers and other community leaders. For instance, in some cultures to pat a child on the head is an insult. An investigator needs to know as much as possible about the culture of the child who is to be interviewed. Religious practices and the role men, women and children play in various cultures were discussed.
This was followed up with a meeting between prosecutors, police officers, social workers and members of our Southeast Asian community. Members of its community expressed concerns that if they discipline their children, they will be arrested. We explained what does and does not constitute physical abuse under Minnesota law.
EDUCATING THE PUBLIC
Sixth, we recently began, with the support of local youth groups, a year long media campaign to educate the public about child abuse. We adhere to the African proverb that it takes a whole village to raise one child. Accordingly, no campaign against child abuse can be successful without the support of everyone in the community. To this end, prosecutors and social workers prepared monthly newspaper ads explaining what child abuse is, how to report suspected abuse and how to prevent abuse. In one ad, we listed alternatives to lashing out at your kid. These alternatives include the following:
1. Take a deep breath - and another - then remember you are the adult.
2. Close your eyes and imagine you're hearing what your child is about to hear.
3. Press your lips together and count to 10, or better yet, count to 20.
4. Put your child in a time-out chair. (Use the rule: one time-out minute for each year of age.)
5. Put yourself in a time-out chair. Think about why you are angry: is it your child or is your child simply a convenient target for your anger?
6. Phone a friend.
7. If someone can watch the children, go outside and take a walk.
8. Take a hot bath or splash cold water on your face.
9. Hug a pillow.
10. Turn on some music; maybe even sing along.
11. Pick up a pencil and write down as many helpful words as you can think of. Save the list.
38
A local physician copied this ad and placed it in the waiting area and examining rooms at a local family clinic. A local newspaper gave our local youth group a monthly column to address the needs of children and families.
CONCLUSION
As a result of these and other efforts, more Cottonwood County child abusers have been charged, convicted and imprisoned in the past three years than in the previous 12 years. Although it cannot be proven with statistics, we are optimistic that our prevention efforts have spared numerous children from abuse. The credit belongs to everyone who stood up and proclaimed that children living in the shadows are as loved as those residing in the day light.
Robert Kennedy once said that although few of us will have the greatness to bend history itself, each of us can send a tiny ripple of hope. Today, in Cottonwood County and in rural communities across the nation, abused children have more hope than ever before. May we never lose our resolve to keep this hope alive.
39
Additional Suggested Reading
Anatomical Dolls
Boat B.W. & Everson, M.D. (1994). Putting the anatomical doll controversy in perspective: An examination of the major uses and criticisms of the dolls in child sexual abuse evaluations. Child Abuse & Neglect, 18(2), 113-129.
Renier, A., & Simkins, L. (1996). An analytical review of the empirical literature of
children's play with anatomically detailed dolls. Journal of Child Sexual Abuse, 5(1), 21-45.
Child Development
Bussey, K., Goodman, G. S., Saywitz, K. J., & Stewards, M. S. (1993) Implications of
developmental research for interviewing children. Child Abuse & Neglect, 17(1) 25-38.
Walker, A. G. (1999). Handbook on questioning children: A linguistic perspective (2nd edition.) American Bar Association's Center on Children and the Law.
Cavanagh Johnson, T. (2003). Understanding Children's Sexual Behaviors: What's Natural and Healthy [Booklet].
Child Witnesses
Camparo, L., & Saywitz, K. (1998). Interviewing child witnesses: A developmental perspective. Child Abuse & Neglect, 22(8), 825-843.
Cultural Issues
Bottoms, B. L., Goodman, G. S., Shaver, P. R., & Qin, J. (1996). Religion and child abuse. The APSAC Advisor, 9(2).
Fontes, L. (1993). Sexual abuse in nine North American cultures: Treatment and prevention. Newbury Park, CA: Sage.
Heras, P. (1992). Cultural considerations in the assessment and treatment of child sexual abuse. Journal of Child Sexual Abuse, 1(3). Custody/Divorce
40
Boss, D.C. (1992). Assumptions about child sexual abuse allegations at or about the time of divorce: A commentary. Journal of Child Sexual Abuse, 1(2).
Schudson, C. B. (1992). Antagonistic parents in family courts: false allegations or false assumptions about true allegations of child sexual abuse? Journal of Child Sexual Abuse, 1(2).
Interview Techniques
Garven, S., & Wood, J. M. (2000). How sexual abuse interviews go astray: implications for prosecutors, police, and child protection services. Child Maltreatment, 5(2), 109-118.
Legal
Lyon, T. D., & Saywitz, K. J. (1999). young maltreated children's competence to take the oath. Applied Developmental Science, 3(1), 16-27.
Lyon, T. D. (1996). Assessing children's competence to take the oath: research and recommendations. The APSACAdvisor, 9(1).
Process of Disclosure
Campis, L. B., Demaso, D. R.., & Hebden-Curtis, J. (1993). Developmental differences in
detection and disclosure of sexual abuse. Journal of American Academy of Child and Adolescent Psychiatry, 32(5) 920-924.
Dalenberg, C. J., & Dunkerley, G. K. (1999). Secret-keeping behaviors in black and white children as a function of interviewer race, racial identity and risk for abuse. Maltreatment in Early Childhood: Tool for Research-Based Intervention. Haworth Press, Inc.
Bradley, A. R., & Wood, J. M. (1996). How do children tell? The disclosure process in child sexual abuse. Child Abuse & Neglect, 20(9), 881-891.
Sauzier, M. (1989). Disclosure of child sexual abuse: for better or for worse. Psychiatric Clinics of North America, 12(2).
Briere, J., & Elliott, D. M. (1994). Forensic sexual abuse evaluations of older children:
Disclosures and symptomatology. Behavioral Sciences and the Law, 12,261-277.
41
Process of Inquiry/Instruction
Bartosik, S., Beer, J., Geddie, L.F., & Wuensch, K.L. (2001). The relationship between interview characteristics and accuracy of recall in young children: Do individual differences matter? Child Maltreatment, 6(1), 59-68.
Dowden, C, Peterson, C, & Tobin, J. (1999) Interviewing preschoolers: Comparisons of yes/no and wh- questions. Law and Human Behavior, 23(5), 539-555.
Suggestibility/Memory
Bruck, M., & Ceci, S. J. (1999). The suggestibility of children's memory. Annual Review of Psychology, (50)419.
Bruck, M., & Ceci, S. J. (1995). Jeopardy in the courtroom: A scientific analysis of children's testimony. American Psychological Association, Washington DC.
Lyon, T.D. (1999). The new wave in children's suggestibility research: A critique. Cornell Law Review, 84(4).
42
A Selected Bibliography and Resources on Child Sexual Abuse
Compiled by CornerHouse
Intervention, Investigation & Court Testimony
Goldstein, S. (1987). The sexual exploitation of children: A practical guide to assessment, investigation and intervention. CRC Series in Practical Aspects of Criminal and Forensic Investigations. Boca Raton: CRC Press.
► Written by a law enforcement investigator, it covers various aspects of criminal child sexual abuse investigation.
MacFarlane, K, & Waterman, J. (1986). Sexual abuse of young children. New York: Guilford Press.
► Written by a pioneer in the field, contains sections on the scope of the problem, evaluation of young children, social and legal considerations, and treatment of young children and families. Includes a section on helping parents cope with non-familial molestation.
Zaragoza, M., Grapham, J., Hall, G., Hirschman, R., & Ben-Porath, Y. (Eds.). (1995). Memory and testimony in the child witness, Thousand Oaks, CA: Sage Publications.
► Set of articles by experts in the field on the nature of children's eyewitness testimony, improving children's testimony, and social implications.
Dynamics and Treatment
Barbaree, H., Marshall, W., & Hudson, S. (Eds.). (1993). The juvenile sex offender. New York: Guilford Press.
► Examines the juvenile offender, development of sexually assaultive behavior and current types of treatment.
Finkelhor, D. (Ed.). (1986). A sourcebook on child sexual abuse. Newbury Park, CA: Sage Publications.
► Landmark book on the prevalence and effects of sexual abuse; still useful today.
Fontes, L. A. (Ed.). (1995). Sexual abuse in nine North American cultures: Treatment & prevention. Thousand Oaks, CA: Sage Publications.
► Provides overview of sexual abuse in these cultures: African American; Puerto Rican; Asian, Pacific Island and Filipino Americans; Cambodian; Jewish; Anglo American; Seventh Day Adventist; Gay Males; and Lesbians. Includes chapter on culturally informed interventions in child sexual abuse.
43
Heitritter, L., & Vought, J. (1989). Helping victims of sexual abuse: A sensitive, biblical guide for counselors, victims & families. Minneapolis: Bethany House Publishers.
► Contains sections on understanding the abused child, understanding the abused family and helping the adult victim.
Herman, J. (1992). Trauma and recovery. New York: Basic Books.
► Examines the impact and recovery process for victims of Post-traumatic Stress Syndrome, including childhood sexual abuse.
Mendel, M. P. (1995). The male survivor: The impact of sexual abuse. Thousand Oaks, CA: Sage Publications.
► Reports on the findings of the first national survey of male victims of sexual abuse. Discusses the extent of male sexual abuse and its effects.
Summit, R. (1992). Abuse of the child sexual abuse accommodation syndrome. Journal of Child Sexual Abuse, 1(4), 153-163.
Terr, L. (1994). Unchained memories: True stories of traumatic memories, lost and found New York: Basic Books.
► Written by a psychiatrist specializing in childhood trauma. Presents and discusses seven cases of reclaimed memories.
For Mandated Reporters
Center for the Prevention of Sexual and Domestic Violence. What you need to know if a child is being abused or neglected. 936 North 34th Street, Suite 200, Seattle, Washington 98103.
► This is a brochure designed for clergy, lay leaders and volunteers in churches and synagogues.
ETR Associates. PO Box 1830, Santa Cruz, CA 95061. (800) 321-4407; Web site: http://www.etr.org.
► They publish the guide "When Sex is the Subject." A good resource for parents and teachers.
National Center on Child Abuse and Neglect. PO Box 1182, Washington, DC 20013. (301)251-5157.
National Committee for the Prevention of Child Abuse. 332 S. Michigan Avenue, Chicago, IL 60604. (312)663-3520.
Plummer, C. (1984). Preventing sexual abuse: Activities and strategies for those working with children and adolescents. Holmes Beach, FL: Learning Publications.
► Includes curriculum guides for K-6, 7-12 and special populations.
SIECUS. 130 W. 42nd Street, Suite 350, New York, NY 10036. (212)819-9770; Website: http://www.siecus.org.
44
► This organization has extensive booklets, bibliographies, teacher materials, and a Web site for parents.
Tower, C.C. (1992). The role of educators in the prevention and treatment of child abuse and neglect. Washington, D.C.: National Clearinghouse on Child Abuse and Neglect, U.S. Dept. of Health and Human Services, User Manual Series.
► Includes information on talking with children and parents, what to do, what not to do, as well as other good information on physical and sexual abuse and neglect.
For Parents and Caregivers
Byerly, C. (1985). The mother's book: How to survive the incest of your child. Dubuque, IA: Kendall/Hunt Publishing.
► Provides information and support for mothers of incest victims. Includes chapters on responding to disclosure, parenting issues, cultural issues, and religious perspectives.
Haffher, D.W. (1999). From diapers to dating: A parent's guide to raising sexually healthy children. Newmarket Press, New York.
Indian Child Welfare Council. (1990). Walking in your child's moccasins. Portland, OR: National Indian Child Welfare Association.
► Booklet about child abuse and neglect for parents and caregivers of Native American children.
Ledray, L.E. (1986). Recovering from rape. New York: Henry Holt and Company.
► Provides practical advice on overcoming the trauma and coping with police, hospitals, and court for survivors of sexual assault and for their families and friends.
Rape, Abuse, and Incest National Network. 635 B Pennsylvania Avenue, SE, Washington, DC 20003. (800) 656-HOPE; Web site: http://www.rainn.org.
► This organization can help you deal with cases of rape, sexual abuse and incest.
SDECUS. 130 W. 42nd Street, Suite 350, New York, NY 10036. (212)819-9770; Website: http://www.siecus.org.
► This organization has extensive booklets, bibliographies, teacher materials and a Web site for parents.
For Adult Survivors of Sexual Abuse
Bass, E. & Thornton, L. (Eds.). (1983). / never told anyone: Writings by women survivors of child sexual abuse. New York: Harper & Row.
► True stories of sexual abuse by fathers, other relatives and strangers. Designed to help adult survivors break the silence and begin healing by learning of others' experiences.
45
Barnes, P.D. (1989). The woman inside: From incest victim to survivor. Racine, WI: Mother Courage Press.
► A workbook for women recovering from the effects of incest.
Lee, S. (1995). The Survivor's Guide. Thousand Oaks, CA: Sage Publications.
► For adult sexual abuse survivors. Focuses on the effects of abuse and recovery.
Middleton-Moz, J. & Dwinell, L. (1986). After the tears: Reclaiming the personal losses of childhood Deerfield Beach, FL: Health Communications, Inc.
► Written for adult children of alcoholics who may have experienced a variety of abuse, including sexual abuse. Focuses on grief resolution as part of a recovery process.
For Children & Adolescents
Drake, E. D.; Gilroy, A. E.; & Roane, T. H. Working together: A team effort. Child Care Publications.
► Available from: Child Care Publications (904) 472-4654. This is a book written for boys who are victims of sexual abuse.
Freeman, L. (1986). Loving touches: A book for children about positive, caring kinds of touching. Seattle: Parenting Press..
► Available from: Parenting Press, P. O. Box 15163, Seattle, WA 98115. Describes touching as something that every child needs and shows children positive ways to have this need met. Suitable for very young children.
Hindman, J. (1983). A very touching book Ontario, OR: AlexAndria Associates.
► Can be ordered from AlexAndria Associates, 911 SW 3rd St., Ontario, OR 97914. Excellent book for children on touching, feelings and what to do if there is "secret touching." Introduces and uses correct terms for genitals.
Mather, C. (1994). How long does it hurt? A guide to recovering from incest and sexual abuse for teenagers, their friends, and their families. San Francisco: Jossey-Bass Publishers.
► This is a step-by-step recovery guide for teenagers who have been or are being sexually abused.
Peltier, M. (1994). Breaking the silence: Kids against child abuse. Arnold Shapiro Productions in cooperation with USAA.
► Videotape for children and their parents. With the help of animation, four young children tell what happened to them and how they got help. Provides information on how to stop and prevent child abuse. Emphasizes importance of child telling a trusted adult.
Pucci, L, and Copen, L. (1995). Finding your way: What happens when you tell about abuse. Kenosha, WI: Tree of Serenity Press.
46
► Available from: Tree of Serenity Press, 4109 67th Street, Kenosha, WI 53142. Written for older children and adolescents (ages 9-18) who may have been sexually, physically or emotionally abused, although the primary focus is on sexual abuse. Discusses telling about abuse, what is involved in investigation and court procedures from the child's perspective, and the healing process.
Williams, J. (1983). Redflag green flag people. Fargo, ND: Richtman's Printing
► Available from: Red Flag Green Flag Resources, Rape & Abuse Crisis Center, P. O. Box 2984, Fargo, ND 58108-2984. Phone: (800)627-3675. Thirty-page coloring book introduces concepts of personal safety to children ages 3-5. Materials and curriculum guides for kindergarten and elementary age children are also available.
47
Allegations of Sexual Abuse Amidst Divorce/Custody Disputes
48
Pre-Test on Divorce/Custody *
Please answer the following questions either true or false:
1. Media attention given to parents battling one another and the courts over accusations and denials of child sexual abuse have dramatized the seriousness of allegations of child sexual abuse made in the context of divorce/custody disputes.
True False
2. Allegations of sexual abuse in child-custody disputes are common. True False
3. Parents, especially mothers, often fabricate sexual abuse allegations in child-custody disputes.
True False
4. The "backfire" scenario is when courts award custody to the parent accused of sexual abuse due to the other parent's refusal to allow unsupervised access to the child.
True False
5. A parent accused of child sexual abuse is more likely to confess if his/her family is intact rather than if the family is separated.
True False
6. If a case of reported child sexual abuse is categorized as either unsubstantiated or unfounded, it always means that the act did not happen.
True False
7. It's possible that cases that are substantiated or founded may in fact not be true abuse cases.
True False
49
8. The proper approach for an assessment worker and/or an investigator is to regard the child sexual abuse allegation made in the context of a custody dispute the same as if it were made against a person outside the family or a person inside an intact family.
True False
9. There are systemic problems in the court system which may lend to the myth that the parent fabricated the allegation.
True False
10. (A) False allegations of sexual abuse in the context of child-custody disputes
do occur.
True False
(B) False allegations of sexual abuse in the context of child-custody disputes represent only a minority of cases.
True False
(C) Deliberate fabrication of sexual abuse allegations occur in only a small percentage of cases arising in the context of child-custody disputes.
True False
♦Adapted from:
Corwiri, D. L. Child sexual abuse and custody disputes. Ross Roundtables.
David W. Lloyd, D. W. Contention in custody cases: Legal perspective. Ross Roundtables.
50
Fact Sheet: Child Sexual Abuse Allegations in Custody and Visitation Disputes*
How frequent are child sexual abuse (CSA) allegations in divorce custody disputes?
In a 1990 study of9,000 divorces in 12 states, CSA allegations were made in less than 2% of contested divorces involving child custody. This study was commissioned by the Association of Family and Conciliation Courts.
No reliable national study documents either an increase or decrease in CSA allegations in custody disputes since 1990.
Who makes these allegations?
In the 1990 study cited above,
Mothers accused fathers in 48% of cases
Mothers accused stepfathers or others in 19% of cases
Fathers accused mothers in 6% of cases
Fathers accused stepfathers or others in 16% of cases
Third parties accused fathers, mothers, or others in 11% of cases
How often are these allegations intentionally false?
Determining which allegations are false is often extremely difficult, and few reliable studies on this topic are available. The incidence of intentionally false reports generally appears to be 5% to 8% of all cases.
How often are these allegations "unfounded"?
The large-sample study cited above found that CSA allegations in custody disputes were substantiated about as frequently as all other CSA allegations.
What does "unsubstantiated" or "unfounded" mean?
"Unsubstantiated" and "unfounded" do not mean "false." They mean, "Not enough evidence to make a determination." Cases may be unfounded because:
The caseworker has no time to investigate The alleged victim is too young to testify
The suspicion has been reported previously and determined to be unfounded, and is not re-investigated
♦Adapted from:
Goldstein, S. L. & Tyler, R. P. (1998). Sexual abuse allegations in custody cases: Difficult decisions in divisive divorces. APS AC Advisor. 11(31. 15-18.
51
Source of Allegations of Child Sexual Abuse in Custody and Visitation Disputes*
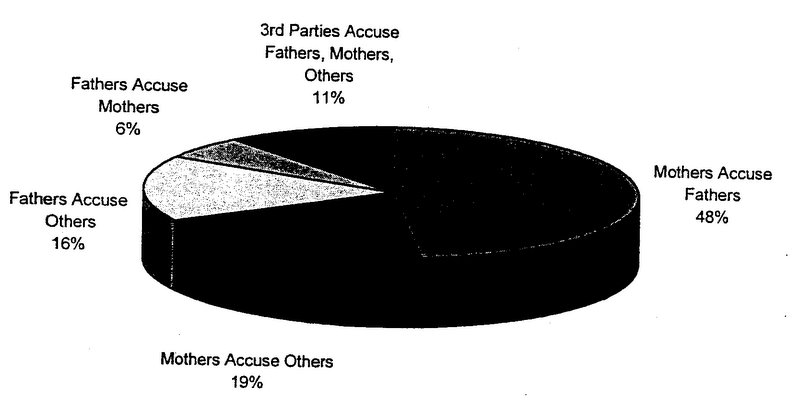
*From:
Thoennes N & Tjaden PG. (1990). The extent, nature, and validity of sexual abuse allegations in custody/visitation disputes. Child Abuse and Neglect 141151-163.
52
Characteristics of a Child-Focused, Non-Fabricating Parent
Versus
Characteristics of an Ex-Spouse-Focused, Suspect Parent
*This is not a check list - just some guidelines
1. Expresses remorse for not protecting the child sufficiently to prevent the abuse.
Versus
Expresses little or no remorse for child only vindictiveness towards ex-spouse.
2. Willing to consider other possible explanations for the behavior or statements that aroused their suspicion.
Versus
Unwilling to consider any other explanation of the child's statements, behavior, or symptoms.
3. Willing to have the child interviewed without being present.
Versus
Insists on being present when the child is interviewed and prompts her when she is questioned about the abuse.
4. Concerned about the impact on the child if he/she has to testify.
Versus
Is eager for the child to testify at all costs.
5. If allegations cannot be verified, they are willing to let go of the investigatory process so long as the child's well-being can be monitored through therapy or some other process.
Versus
53
Shop for other professionals who will verify her suspicions and involve the child in multiple examinations so the investigation can continue, irrespective of the impact the process is having on the child.
Adapted from:
Bresee P., Stearns, G. B., Bess, B. H. & Packer, L. S. (1986). American Journal of Orthopsychiatry. 56(4).
54
Reprinted with permission from:
Faller, K, Corwin, D. L. & Olafson, E. (1993). Literature review: Research on false allegations of sexual abuse in divorce. The APSAC Advisor 6(3). 7-10.
Literature Review:
Research on False Allegations of Sexual Abuse in Divorce
Kathleen Coulborn Faller, David L. Corwin, and Erna Olafson
Introduction
The statement, "There is an epidemic of false allegations of sexual abuse in divorce cases," is regarded by some as a truism. The argument is that women seeking to win custody of their children, to cut off the father's visitation, or to wreak vengeance on former spouses, falsely accuse them of child sexual abuse (Mantell, 1988; Renshaw, 1985; 1986). Such is the assertion of accused fathers, their attorneys (Gordon, 1985), and their expert witnesses (Blush and Ross, 1986; Gardner, 1989). Moreover, the media have supported and broadcast these views, and many professionals with mandated responsibility for these cases, including child protection workers, law enforcement personnel, and, most importantly, judges, have come to believe that abuse allegations during divorce are likely to be false.
Are there any empirical findings that lend credibility to the view that most allegations of child abuse in divorce are false? In this article, literature addressing this issue will be critically reviewed, looking specifically at data cited, sample size, any sample biases, and the criteria employed to determine the veracity of the allegation.
Studies Providing No Data
Writers holding the most extreme positions and promulgating new "syndromes" provide no data to support their statements (Blush and Ross, 1986; Gardner, 1987).
Blush and Ross have propounded the Sexual Allegations in Divorce (SAID) Syndrome, the overwhelming majority of which they assert are false. These false allegations are fostered by mothers, whom Blush and Ross label psychotic or hysterical (dominated, dominating, or "justified vindicators"). They advise that almost no weight should be given to any statement made by the child, and in practice they may not even interview the child. However, Blush and Ross maintain, great weight should be given to the fact that these allegations are made by mothers who wish to restrict their ex-partners' access to their children (Ross, 1988). Blush and Ross find fathers much less likely to make false allegations, and describe those who do as rigid and hypercritical of their estranged wives. Falsely accused men are also described as inadequate, dependent, and passive, descriptors the authors also apply to incest perpetrators.
Since no data are provided, there is no way to evaluate the SAID Syndrome, other than to note that the admonition to put little weight on children's accounts is contrary to general practice (see Conte et al., 1991).
* APSAC is a multidisciplinary society for professionals in the field of child maltreatment. For more information, call (312) 554-0166.
55
Perhaps even stronger views are held by Gardner (1987; 1989; 1991; 1992), who has defined the Parental Alienation Syndrome (PAS), which is manifest in children who "view one parent as all good and the other as all bad." These children have been "programmed by their mothers to hate their father and to subject him to a campaign of denigration" (Gardner, 1992, p. 160). Among the material the mother sometimes also programs the child to believe is that the father has sexually abused him/her. When an allegation arises after a dispute over custody, Gardner believes it possesses a "high likelihood of being false" (Gardner, 1991, p. 4).
A companion to the PAS is the Sexual Abuse Legitimacy Scale (SALS, Gardner, 1987). The present version (1992) contains 84 differentiating criteria, 24 of which apply to the alleged offender, 30 to the child, and 30 to the mother. Many of these criteria relate specifically to allegations of abuse in divorce. For example, if one finds, in examining the mother, "the presence of a child custody dispute and/or litigation," "enlistment of the services of a 'hired gun' attorney or mental health professional," or "history of attempts to destroy, humiliate, or wreak vengeance on the accused," her allegations are less likely to be true, according to Gardner.
Gardner presents no data to validate either the PAS or the SALS. Therefore, the utility of the scales cannot be evaluated. Most of Gardner's writing on these topics is not peer reviewed and is published through his own press.
Studies Involving Small Samples
The first and oft-cited clinical study of false allegations of sexual abuse in divorce involved a single case and reference to a second one (Kaplan and Kaplan, 1981). In the case, described in detail, an 11-year-old boy and his 5-year-old sister made allegations against their father and paternal grandparents. Both children had testified numerous times in court about the abuse and persisted in their accusations when challenged. Indeed, the Kaplans describe one particularly stormy session in which the boy is confronted simultaneously by the paternal grandparents and one of the Drs. Kaplan. Because, during this session, the boy partially recanted and said he had only been anally penetrated once instead of numerous times, the Kaplans conclude that his allegation is false. His partial recantation also led them to doubt the sister's account even though, in addition to her statements, she had a number of behavioral and emotional symptoms of sexual victimization. The Kaplans propose the possible dynamic offolie a deux as an explanation for the children's allegations, despite the fact there was no delusional thinking diagnosed in either child, the mother, or the maternal grandparents, who were supportive of the allegations, and despite the fact that the allegations originated with the children rather than a dominant adult.
Another frequently quoted study is that of Schuman (1986), who cites seven cases determined to be false on the basis of "psychodynamic formulation" and court determinations, out of an unknown number seen in his practice of probate and family court cases. Six of these were sexual abuse allegations against a father or stepfather; the seventh was a physical abuse case. The psychodynamic explanation for the false allegations was regression by the child and the accusing adult; in addition, in some instances (Schuman does not say how many) this adult retracted the allegation. This study is limited by its small sample size and by the lack of an empirical basis for the criteria Schuman uses to determine that allegations are false.
A study that has excited quite a lot of controversy is one reported by Green (1986) involving 11 cases from his practice, four of which (36%) he believed to be false. From these four cases, he generates criteria indicative of a false allegation, including easy disclosure, no evidence of negative affect, use of adult sexual terminology, checking with the accusing parent (mother) during the interview, and an ability to confront the father with the accusation. Falsely accusing mothers are described as hysterical and paranoid.
56
Green's conclusions were challenged because of the size and bias of his sample, and because one of his "false" cases was deemed possibly valid by two other experts in child sexual abuse (which would reduce his rate of false cases to 27%). His paper occasioned a rebuttal article (Corwin, Berliner, Goodman, Goodwin, and White, 1987) as well as a letter to the editor of the journal that published the original article, challenging its findings (Hanson et al., 1988). Among other things, Corwin and colleagues point out that there is a difference between a false (no abuse) and an unsubstantiated case (a null finding). In addition, they note that marital dissolution may increase the risk of sexual abuse and increase the likelihood of disclosure of pre-existing incest.
Benedek and Schetky (1985) also present findings from their private practices. They were interested in studying the characteristics of false allegations in divorce, and Benedek (1987) reports screening at intake to include suspected false cases and to exclude ones that appeared to be true. Fourteen of the 18 cases they assessed involved custody or visitation disputes in the context of divorce (four involved other issues related to custody). The authors thought that 10 of their cases were false (71% of 14 and 56% of 18). Not surprisingly, since they screened for false cases, this is the highest false allegation rate reported by any author presenting case data. All but one of the allegedly false allegations were made by mothers. It is not clear what criteria Benedek and Schetky used to determine that allegations were false; among the explanatory factors they cited were that the mother suffered from psychiatric disturbance ("paranoia" was the diagnosis most frequently mentioned by the authors), or wished to exclude their ex-spouses from their lives, were being vindictive, or were "crying wolf." A much larger study (576 cases ) of sexual abuse cases referred to child protective services provided findings relevant to the issue of sexual abuse and divorce (Jones and McGraw, 1987). Criteria employed in classifying the cases as likely true or likely false consisted of source of report, child's emotional state, physical evidence, confessions, polygraph results, and court role. Of the 5% of cases which a team of sexual abuse experts determined were "fictitious" allegations by adults, a large proportion involved contested custody or visitation. These findings suggest that false accusations are very rare generally, but may be more common in the context of custody disputes. In a subsequent study by Jones and Seig (1988), 20 divorce cases involving accusations of sexual abuse from the Kempe Center were evaluated using the Jones and McGraw (1987) criteria to ascertain the rate of fictitious allegations. Four cases (20%) were determined to be fictitious, 14 (70%) reliable, and 2 (10%) uncertain. In this study, the authors observed that factors thought to be characteristic of false allegations were noted in the reliable cases, and characteristics expected in reliable cases were noted in the fictitious ones.
Using the criteria developed by Jones and McGraw (1987) and used by Jones and Seig (1988), McGraw and Smith (1992) re-examined 18 cases referred to Boulder County Protective Services involving sexual abuse allegations in the context of divorce, all but one of which had been unfounded after CPS investigation. The results of this re-examination were that eight cases (44.4%) were founded, seven cases (39%) had insufficient information or unsubstantiated suspicion, and three (16.5%) were fictitious (one from a child and two from adults). The authors admonish investigators and clinicians to keep an open mind when investigating such cases, rather than assuming that they will be false.
Studies Comparing Divorce Cases to Other Sexual Abuse Cases
Two studies compare results from divorce and non-divorce cases. Paradise, Rostain, and Nathanson (1988) examined 31 cases (25 from Children's Hospital of Philadelphia and six from the first author's private practice), 12 of which involved divorce. Those cases involving divorce were significantly less likely to be substantiated: 67% substantiation rate in divorce cases vs. 95% substantiation rate in cases not involving divorce. In addition, children in the divorce group were significantly younger (5.4 years
57
vs. 7.8); this age difference may have affected substantiation rates, since cases involving younger children may be generally more difficult to substantiate (Thoennes and Tjaden, 1990). Hlady and Gunter (1990) examined the records of 370 children seen at the Child Protection Service Unit at British Columbia Children's Hospital. One hundred seventeen children were primarily referred for alleged physical abuse, and 253 for alleged sexual abuse. Forty-one children were the objects of custody disputes. Surprisingly, children involved in custody disputes were more likely to exhibit physical findings (75% had findings of physical abuse, 17.6% had findings of sexual abuse) than were children not involved in custody disputes (43.6% showing findings of physical abuse, 15% of sexual abuse). Generalizations from these data must be cautious, since the number of custody cases with allegations of physical abuse was small, and the difference on sexual abuse cases was not significant. However, these data suggest that sexual abuse allegations made in the context of divorce are at least as likely to have the corroboration of medical findings.
More studies comparing commonly evaluated characteristics of sexual abuse cases in divorce and other contexts would be very useful.
Studies Involving Larger Samples
To date, there are two pieces of research with samples larger than 100 cases. Faller (1990) studied 136 cases involving divorce that were referred to the University of Michigan Interdisciplinary Project on Child Abuse and Neglect, which includes a tertiary care program for evaluation of child maltreatment cases. Using criteria derived from a study of confessed cases, Faller determined the likelihood of sexual abuse in her sample. These criteria included (1) description of the sexual abuse; (2) details about the context; and (3) affect congruent with allegations and circumstance. Faller categorized these cases into six groups: cases in which disclosure of apparently true abuse leads to divorce (N=l 1; 8.1%); cases in which divorce leads to disclosure of apparently true abuse by the child or belief by the parent (N=26; 19.1%); cases in which divorce leads to sexual abuse (N=52; 38.2%); cases in which apparently false allegations arise in an atmosphere of acrimony surrounding the divorce (N=19; 14%); cases in which false allegations may have been made (N=12; 8.8%); and cases in which other dynamics were at work (N=16; 11.8%). Of the 19 cases involving apparently false allegations, three appeared to be consciously made; two of these three intentionally false allegations were made by fathers.
By far the most important study to date is that conducted by the Association of Family and Conciliation Courts Research Unit (Thoennes, Pearson, and Tjaden, 1988; Thoennes and Tjaden, 1990). The researchers surveyed 9,000 divorce cases involving custody/visitation disputes from 12 domestic relations courts to determine how many such disputes involve allegations of sexual abuse. The researchers found allegations of child sexual abuse in less than two percent (169) of these cases. In 129 cases, the question of sexual abuse was addressed by the domestic relations court. Accusations were made by mothers (67%), fathers (28%), and third parties (11%). Fewer than half of cases involved mothers making accusations against the fathers of children.
Using the Child Protective Services determination and/or the report of a court-appointed mental health evaluator as the criteria for substantiation, the researchers found that 50% of cases were likely, 33% were unlikely, and 17% were uncertain (which included cases in which two evaluators held different opinions). They also attempted to discern the motivation for unlikely reports and found 58 cases in which the case material addressed that issue. In eight cases, child protective service workers thought the allegation was maliciously made. Factors associated with cases being classified as unlikely or uncertain were younger age of the child, a single incident alleged, non-intrusive sexual behavior, a single report, a report less than two years since the filing for divorce, and animosity between the parents.
58
Conclusions
On the basis of the research that has been conducted so far, it is difficult to support an assertion that there are high rates of false allegations of sexual abuse consciously made by mothers in divorce situations.
There is no way to evaluate authors' opinions not supported by data. Thus all that can be said about the SAJD Syndrome and the Parental Alienation Syndrome is that they express the authors' opinions. Moreover, the language used in both suggests a bias against mothers concerned about sexual abuse of their children.
The remainder of the research can be evaluated regarding possible sample biases, sample size, and criteria used to determine that the allegation is false.
With the exception of the research supported by the Association of Family and Conciliation Courts (Thoennes and Tjaden, 1988; Thoennes and Tjaden, 1990) and that by Paradise and colleagues (1988), all of the studies cited rely on cases from a single source. A single site or source may introduce biases based upon geography, the authors' selection criteria, and the reputation of the clinician or the site. Selection criteria include such factors as Benedek's screening for cases she thought might be false, or Faller's taking cases referred by another agency. Payment source for the service may also determine the sorts of cases seen at a particular site. In addition, cases seen in private practices are likely to differ from those seen at an agency or at a hospital.
Sample size is also very important in weighing the utility and potential validity of findings. It is very difficult to draw any conclusions from samples smaller than 20 cases. Particularly problematic is the situation in which the writer draws conclusions about characteristics of false allegations from a subset of a small sample, as does Green (1986).
The most difficult problem in evaluating research on allegations of child sexual abuse is evaluating the criteria researchers use to assess the veracity of allegations. To test these criteria, researchers need to see if they are in fact reflected in a sample of cases proven false or true by some independent measure (for example, that the offender never had access to the victim, or, alternatively, that the offender gave a complete, detailed confession). Since such samples are hard to find and indeed may be unrepresentative, research on the veracity of child sexual abuse allegations cannot draw upon them. Most writers use their clinical judgment, the consensus of several clinicians or experts, or a legally supported decision, such as the disposition of the child protection agency, the conclusion of a court-appointed expert, or a judge's opinion. All of these have limitations. Jones' and Seig's (1988) determination that cases thought to be reliable had characteristics of false reports and vice versa is illustrative. So is the Association of Family and Conciliation Courts' classification of cases as "uncertain" when two opinions disagreed.
Moreover, there is a fair amount of disagreement among writers about characteristics of false allegations. Indeed, one professional's indicator of a false allegation may be another's indicator of a true one. In addition, some criteria lend themselves to a variety of interpretations, either in the context of a single case, or depending upon the case.
When the research is examined critically, the strongest study is that conducted by the Association of Family and Conciliation Courts, because of its large sample, its use of multiple sites, and the fact that cases are fairly representative of the total population of divorce cases with disputes over custody and visitation. Its findings indicate that sexual abuse allegations do occur in the context of divorce, but the overwhelming majority (98%) of disputed custody cases do not involve sexual abuse accusations. Moreover, although the majority of charges are brought by mothers, by no means all are. The predominance of women as accusers and men as accused is consistent with the finding that the majority of offenders are men. This study and that of Faller contradict the assertion by others that
59
Where the Association of Family and Conciliation Courts may be weaker than other studies is in the criteria it used to judge the veracity of an allegation: the child protective services determination or a court-appointed mental health professional's opinion. Perhaps criteria such as those based on a consensus of experts or a collaborative decision (Jones and McGraw, 1987; Jones and Seig, 1988; McGraw and Smith, 1992) or derived indirectly from cases substantiated by confession (Faller, 1990) are more accurate. Interestingly, substantiation rates tend to be higher in such studies and uncertainty rates lower.
Altogether 11 data-based articles about sexual abuse allegations in divorce are cited here. This number is too small to draw more than tentative conclusions. Moreover, characteristics of allegations in divorce may be influenced by increased public education and experience regarding sexual abuse, so that samples that are just five years old may not reflect current caseloads. Perhaps the likelihood of a parent making a false allegation in divorce has increased because of greater awareness of sexual abuse and of the potential power of an allegation. Conversely, adults may be cognizant of the recent outcomes in such cases. These include disbelief by the court or refusal to hear evidence of sexual abuse, incarceration of the parent who refuses visitation, loss of custody by the parent alleging sexual abuse, and negative experiences of parents, who with their children may go so far as to enter the "underground" to avoid court decisions. This knowledge may result in parents becoming less likely to raise a legitimate concern about sexual abuse because the legal consequences may further traumatize a child and family without stopping the abuse.
References
Benedek, E. Court Tstimony. E. Morgan v. E. Foretich, V. Foretich, and D. Foretich. Alexandria, VA: United States District Court, February 18, 1987.
Blush, G., Ross, K. Sexual Allegations in Divorce: The SAID Syndrome. Unpublished manuscript available from the Psychodiagnostic Clinic, Macomb County Circuit Court, Mt. Clemens, MI, 1986.
Coote, J., Sorenson, E., Fogarty, L., Dalla Rosa, J. Evaluating Children's Reports of Sexual Abuse: Results from a Survey of Professionals. American Journal of Orthopsychiatry, 1991, 61:2.
Corwin, D., et al. Child Sexual Abuse and Custody Disputes: No Easy Answers. Journal of Interpersonal Violence 1987,2(1): 91-105.
Faller, K. Criteria for Judging the Credibility of Children's Statements about Their Sexual Abuse. Child Welfare 1988, 67(5):3 89-401.
Faller, K. Possible Explanations for Child Sexual Abuse Allegations in Divorce. American Journal of Orthopsychiatry 1991, 61(1):86-91.
Gardner, R. Differentiating between Bona Fide and Fabricated Allegations of Sexual Abuse of Children. Journal of the American Academy of Matrimonial Lawyers 1989, 5:1-25.
Gardner, R. The Parental Alienation Syndrome and the Differentiation between Fabricated and Genuine Child Sexual Abuse. Cresskill, New Jersey: Creative Therapeutics, 1987.
Gardner, R. True and False Allegations of Child Sex Abuse. Cresskill, New Jersey: Creative Therapeutics, 1987.
Gardner, R. Sex Abuse Hysteria: Salem Witch Trials Revisited. Cresskill, New Jersey: Creative Therapeutics, 1991.
60
Gardner, R. True and False Allegations of Child Sex Abuse. Cresskill, New Jersey: Creative Therapeutics, 1992.
Gordon, C. False Allegations of Abuse in Child Custody Disputes. Minnesota Family Law Journal 1985, 2(14):225-228.
Green, A. True and False Allegations of Sexual Abuse in Child Custody Disputes. Journal of the American Academy of Child Psychiatry 1986,25:449-455.
Hanson, G. The Sex Abuse Controversy: Letter to the Editor. Journal of the American Academy of Child and Adolescent Psychiatry 1988, 27:258.
Hlady, L., Gunter, E. Alleged Child Abuse in Custody Access Disputes. Child Abuse and Neglect 1990, 14(4):591-594.
Jones, D., McGraw, M. Reliable and Fictitious Accounts of Sexual Abuse to Children. Journal of Interpersonal Violence 1987,2(l):27-45.
Jones, D., Seig, A. Child Sexual Abuse Allegations in Custody or Visitation Cases: A Report of 20 Cases. In: B. Nicholson and J. Bulkley (Eds.), Sexual Abuse Allegations in Custody and Visitation Cases. Washington, DC: American Bar Association, 1988.
Kaplan, S., Kaplan, S. The Child's Accusation of Sexual Abuse during a Divorce and Custody Struggle. Hillside Journal of Clinical Psychiatry 1981, 3(l):81-95.
McGraw, J., Smith, H. Child Sexual Abuse Allegations Amidst Divorce and Custody Proceedings: Refining the Validation Process. Journal of Child Sexual Abuse 1992, l(l):49-62.
Mantell, D. Clarifying Erroneous Child Sexual Abuse Allegations. American Journal of Orthopsychiatry 1988, 58(4):618-621.
Paradise, J., Rostain, A., Nathanson, M. Substantiation of Sexual Abuse Charges When Parents Dispute Custody or Visitation. Pediatrics 1988, 81(6):835-839.
Renshaw, D. Child Sexual Abuse: When Wrongly Charged. Encyclopedia Britannica Medical and Health Annual 1987, 301-303.
Renshaw, D. When Sexual Abuse Is Wrongly Charged. Medical Aspects of Human Sexuality 1985, 19(7):116-121.
Ross, K. SAID Syndrome: Fact or Fallacy. Workshop at Grand Valley State University, Grand Rapids, MI, May 1988.
Schetky, D. Allegations of Sexual Abuse in Child Custody Cases. In: E. Benedek and D. Schetky (Eds.), Emerging Issues in Child Psychiatry and the Law. New York, NY: Brunner/Mazel, 1985, 145-156.
Schuman, D. False Allegations of Physical and Sexual Abuse. Bulletin of the American Academy of Psychiatry and the Law 1986, 14(1):5-21.
Thoennes, N., Pearson, J., Tjaden, P. Allegations of Sexual Abuse in Custody and Visitation Cases. Denver, CO: Association of Family and Conciliation Courts, 1988.
Thoennes, N., Tjaden, P. The Extent, Nature, and Validity of Sexual Abuse Allegations in Custocry/Visitation Disputes. Child Abuse and Neglect 1990,14:151-163.
61
Selected Bibliography on Child Sexual Abuse Allegations Amidst Divorce/Custody Disputes
Compiled by CornerHouse
Benedek, E.P. & Schetky, D.H. (1986). Allegations of sexual abuse in child custody and visitation disputes. In: D.H. Schetky & E.P. Benedek (Eds.), Emerging issues in child psychiatry and the law. New York: Brunner/Mazel, 145-158.
Breese, P.G., Stearns, G., Bess, B. & Packer, L. (1986). Allegations of child sexual abuse in child custody disputes: A therapeutic assessment model. American Journal of Orthopsychiatry. 56(4) 56-568.
Children's Forensic Institute. Sexually abused children's bill of rights. Available from the Children's Forensic Institute, 650 Poydras St., Suite 2030, New Orleans, LA 70130.
Commentary: Berliner, L. (1990). Protecting or harming? Parents who flee with their children. Lloyd D. Disobedience to a judicial order. An inappropriate action. Fisher D. Why parents run. Journal of Interpersonal Violence. 5(1), 119-127.
Corwin, D., Berliner, L., Goodman, G., Goodwin, J. & White, S. (1987). Child sexual abuse and custody disputes: No easy answers. Journal of Interpersonal Violence, 2(1), 91-105.
Faller, K.C. (1990). Understanding child sexual maltreatment. Newbury Park, CA: Sage Publications, 211 -240.
Galtney, L. (1993). Mothers on the run. U.S. News & World Report. June 13.22-33.
Green, A. (1986). True and false allegations of sexual abuse in child custody disputes. Journal of the American Academy of Child Psychiatry, 25, 449-456.
Hopkins, E. (1988). Fathers on trial. New York. January 11.42-49.
MacFarlane, K. (1986). Child sexual abuse allegations in divorce proceedings. In: K. MacFarlane, J. Waterman, et al. (Eds.), Sexual abuse of young children. New York: The Guilford Press, 121-150.
Nicholson, B. (Ed.). (1988). Sexual abuse allegations in custody and visitation cases. Washington, DC: American Bar Association Center on Children and the Law.
Paradise, J., Rostain, A. & Nathanson, M. (1988). Substantiation of sexual abuse charges when parents dispute custody or visitation. Pediatrics. 81(6). 835-839.
Podesta, J.S. & Van Biema, D. (1989) Running for their lives. People. January 23. 70-88.
Thoennes, N. & Tjaden, P.G. (1990). The extent, nature, and validity of sexual abuse allegations in custody/visitation disputes. Child Abuse and Neglect 14(2\ 151 -163.